
Start here · The Captain’s Course
New to krill oil? Read these in order.
- What Is Astaxanthin?
- Is Krill Oil Extracted With Hexane?
- Phospholipid vs. Triglyceride Omega-3s — you’re here
- Does Krill Oil Expire?
- Krill Oil vs. Fish Oil for Joint Pain
- Omega-3s on Ozempic, Wegovy & Mounjaro
Here’s the honest version of this article up front: if you’re already taking a fish oil supplement and tolerating it fine and taking it every day, the form of omega-3 you’re getting probably doesn’t matter enough to switch. The intake is the point. The form is a detail.
But if you’ve tried fish oil and quit — because of the burps, the reflux, the lingering taste, or just the size of the capsule — the form might be exactly the reason you quit. And that makes it worth understanding.
This is an explainer on the three main molecular forms omega-3 supplements come in, what the absorption research actually shows, and when the difference matters enough to care about.
Three Forms, One Fatty Acid
EPA and DHA — the two omega-3 fatty acids your body actually uses — are the same molecules regardless of how they’re packaged. The difference between supplements is the vehicle those molecules ride in from your gut into your bloodstream. There are three common ones:
Ethyl esters (EE). The cheapest form. Created during the concentration process when omega-3s are chemically bonded to ethanol. This is what most bargain-shelf fish oil capsules contain. Your body has to strip the ethanol bond before it can absorb the EPA and DHA, which makes it the slowest and least efficient form. Ethyl esters also depend heavily on dietary fat for absorption — take them on an empty stomach and you lose a significant chunk of the dose.
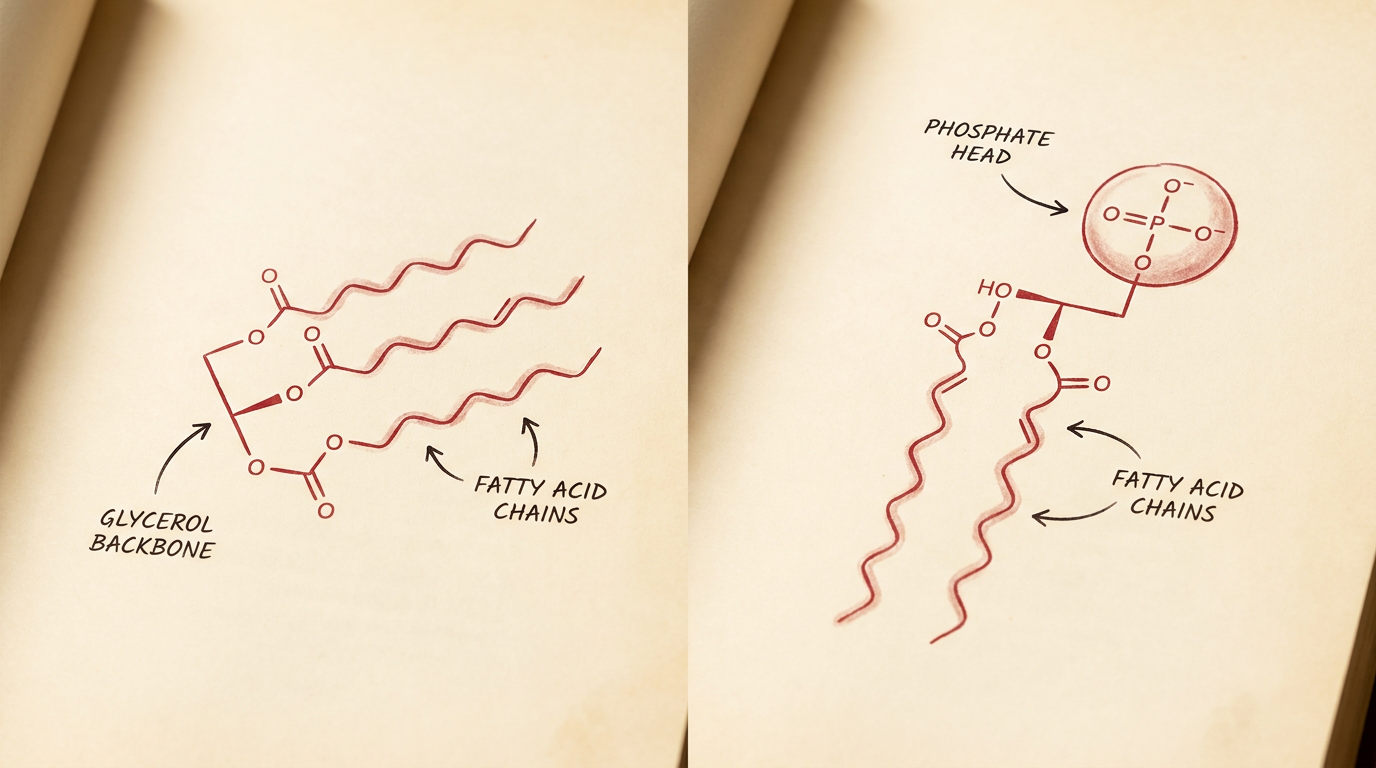
Triglycerides (TG). The natural form found in fish tissue. Three fatty acid chains attached to a glycerol backbone. Your pancreatic lipase knows exactly what to do with this structure — it’s the same form you’d get from eating salmon. Better absorbed than ethyl esters, and the form used in most mid-to-premium fish oil products. Re-esterified triglycerides (rTG) are a concentrated version that tests at the top of the bioavailability charts alongside phospholipids.
Phospholipids (PL). The form found in krill. Instead of three fatty acid chains on a glycerol backbone, you get two fatty acid chains plus a phosphate head group — the same architecture your own cell membranes use. This structural similarity means phospholipid omega-3s integrate into micelles more readily in the gut and don’t require the same enzymatic processing as triglycerides or ethyl esters before absorption (Pham et al., 2024). About 60–70% of the omega-3s in krill oil are bound to phospholipids, with phosphatidylcholine being the dominant carrier.
What the Absorption Studies Actually Show
The bioavailability question has been studied enough times that a rough hierarchy has emerged. The 2025 consensus, drawn from studies published between 2018 and 2024, ranks the forms: rTG ≈ PL > TG > EE. Re-esterified triglycerides and phospholipids sit at the top, natural triglycerides in the middle, ethyl esters at the bottom (MVS Pharma, 2024 review).
A 2024 network meta-analysis — the most comprehensive comparison to date — pooled data across multiple dosage levels and molecular forms. At doses below 2,000 mg (which covers most consumer supplements), krill oil’s phospholipid form showed enhanced area-under-the-curve plasma levels compared to standard fish oil triglycerides (Clinical Nutrition ESPEN, 2024). The advantage was most pronounced at low doses — exactly the range where most people are actually supplementing.
A 2023 randomized, double-blind crossover study compared phospholipid-enhanced fish oil against krill oil directly. The absorption totals were similar, but the profiles differed: the phospholipid forms showed higher, earlier plasma peaks, meaning the omega-3s reached the bloodstream faster (PubMed, 2023).
I want to be careful here. “Better absorbed” is not the same thing as “better for your health.” A 2024 meta-analysis of 64 randomized controlled trials found no significant difference in triglyceride, LDL, HDL, or total cholesterol levels between krill oil and fish oil. The absorption advantage doesn’t always translate into measurably different clinical outcomes — at least not in the endpoints that have been studied so far.
That said, one newer trial pushes back on that conclusion slightly. A 2026 pilot RCT in BMC Complementary Medicine and Therapies randomized 47 patients with hypertriglyceridemia to phospholipid-bound omega-3s (825 mg/day EPA+DHA) or standard omega-3s (903 mg/day EPA+DHA) for 12 weeks. The phospholipid group’s mean triglycerides dropped 9.1 mg/dL; the standard group’s rose 15.2 mg/dL. More notably, 36.4% of the phospholipid group hit the ≤150 mg/dL target versus 13.6% in the standard group (PMC, 2026). It’s a small, pilot study — not proof. But the direction is interesting, and it’s the first head-to-head clinical outcomes trial between the two forms.
The Omega-3 Index Difference
The omega-3 index — the percentage of EPA and DHA in your red blood cell membranes — is arguably a better measure of whether the omega-3s you’re swallowing are actually making it into your cells. The target is 8% or higher. Most Americans sit at 4–5%.
A controlled crossover trial gave 24 healthy volunteers either krill oil or fish oil, each providing 600 mg of omega-3s, for four weeks with washout periods between. Krill oil raised the omega-3 index more than fish oil at the same dose. EPA levels in red blood cells were significantly higher after the krill oil phase. DHA rose compared to control in the krill oil group but didn’t reach significance in the fish oil group (Ramprasath et al., Lipids in Health and Disease, 2013).
An earlier comparative bioavailability study found the same pattern: the highest incorporation of EPA and DHA into plasma phospholipids came from krill oil, followed by re-esterified triglyceride fish oil, then ethyl ester fish oil (Schuchardt et al., 2011).
What this means practically: milligram for milligram, more of the EPA and DHA from phospholipid-bound omega-3s ends up in your cell membranes, where it does its work. A smaller dose of the phospholipid form can move the needle on your omega-3 index as much as a larger dose of triglyceride fish oil.
Why the Form Affects Whether You Actually Take It
This is the part that matters more than any bioavailability chart.
“Fish burps” are the single most cited reason people stop taking fish oil. The mechanism is straightforward: triglyceride oil doesn’t mix with water. It floats on top of your stomach contents. If you get any reflux — and a lot of people do — what comes up tastes like fish. The larger the capsule, the worse the problem, and standard fish oil capsules are not small.
Phospholipids behave differently in the stomach. They’re amphiphilic — one end dissolves in water, the other in fat — which means they emulsify in stomach fluid rather than pooling on top of it. This is the same reason egg yolks emulsify a vinaigrette: the phospholipids in the yolk bridge the oil and water. In practice, this means krill oil supplements are far less likely to repeat on you, and the capsules are typically smaller because the dose doesn’t need to be as large to deliver the same amount of usable EPA and DHA.
For most healthy adults, this is a comfort-of-use difference. Annoying but manageable. But for people with GI sensitivity, people on GLP-1 medications (where nausea and reflux are already daily features), or anyone who has quietly stopped taking fish oil because the experience was unpleasant — this is the difference between a supplement they take and a supplement that sits in the cabinet.
Consistency beats potency. A 500 mg dose you take every day will always outperform a 2,000 mg dose you take when you remember, which will always outperform a 3,000 mg dose you bought once, tried twice, and abandoned.
Astaxanthin: The Bonus You Didn’t Ask About
Krill oil is red. That color comes from astaxanthin, a carotenoid antioxidant that krill accumulate from the microalgae they eat. It’s not added during manufacturing — it’s part of the animal.
Astaxanthin does two practical things in the context of an omega-3 supplement. First, it protects the omega-3 fatty acids themselves from oxidation. Omega-3s are polyunsaturated, which means they have multiple double bonds in their carbon chain — and each one is a site where oxygen can attack the molecule and turn it rancid. Fish oil manufacturers add synthetic antioxidants (usually tocopherols) to slow this down. Krill oil comes with its own antioxidant already built in (Marine Drugs, 2021).
Second, astaxanthin has its own modest evidence base as an anti-inflammatory and antioxidant in human tissue — separate from whatever it does for the oil in the capsule. I wouldn’t buy a supplement for astaxanthin alone, but getting it included in your omega-3 isn’t nothing.
Where the Form Doesn’t Matter
If you eat fatty fish twice a week — real fatty fish, not tilapia — you probably don’t need to think about any of this. Salmon, sardines, mackerel, and anchovies deliver omega-3s in their natural triglyceride form, packaged with the fats and proteins your digestive system evolved to handle. No supplement form will beat that.
If you’re taking a high-quality re-esterified triglyceride fish oil and tolerating it well, your absorption is already near the top of the hierarchy. Switching to krill oil would give you a slightly different absorption profile and smaller capsules, but the practical difference in outcomes is unlikely to be meaningful. Don’t fix what isn’t broken.
If cost is the primary constraint, a standard triglyceride fish oil taken consistently with a meal containing some fat will get the job done. It won’t absorb as efficiently as rTG or phospholipid forms, but the gap narrows when you take it with food, and the most important variable is still whether you take it at all.
Where It Does Matter
The form starts to matter when tolerability is the bottleneck — when you’ve tried fish oil and the experience was bad enough that you stopped. It matters when the dose needs to be small because appetite is low, stomach space is limited, or nausea is already part of the picture. It matters when you want to move the omega-3 index with the minimum effective dose rather than swallowing four large capsules a day.
It matters, in other words, for exactly the people who are most likely to be under-supplemented: the ones who tried and quit.
Captains Krill Oil™ is one option in this space. We make an honest, small-batch phospholipid omega-3 product — always have. But the more important thing than which brand you pick is that you’re getting EPA and DHA from somewhere, in a form you’ll actually take, at a dose that moves your number. The molecule is the point. The vehicle is just how it gets there.
If you want to know where you stand, the omega-3 index test costs about $50 and gives you a real number. Target is 8% or higher. That number matters more than which bottle is on your shelf.
Read next
Don’t take our word for it.
We’re the krill oil from a boat, not a factory — but you should hear it from customers, not from us. Real, unedited reviews from Google and Amazon, each linked to its original.
Read 50+ real Captains Krill Oil reviews →